We have two dogs. One is a Boxer/Shepherd mix rescue that Katie got when she was living alone. She is very protective of Katie (and now, me) and will assume that everyone is a threat until otherwise notified. The other is a Labrador Retriever, who by genetic testing is 100% Lab, though I am certain that she is also 10% Twinkie. Her brothers are hunters, but she is a lover, not a fighter. As such, she will assume that everyone is a friend until otherwise notified. Each dog’s approach to life and other people has its advantages and its disadvantages. Both, though, make a very unambiguous first impression.
First impressions are the core of patient experience. There are places that give registration staff the unofficial title of Director of First Impressions. Other places will refer to their greeters or volunteers as First Impressions Specialists. Getting started on the right foot is essential to healthcare. Everyone familiar with patient experience will say it is much easier to set a good impression than it is to recover from a bad one.
Less obvious, though, is a broader mindset that inadvertently makes it much more difficult to set a good first impression. This belief, which is not unique to healthcare, is that any benefit that a customer or patient gets comes at a cost from the staff or organization. This zero-sum game between patients and staff generally sets the tone for driving patient experience and can make it difficult to successfully drive improvement. For those who don’t know, a zero-sum situation is where gains on one side are off-set by losses on the other, such that when you add up the wins and losses, the sum is zero. While there are positive-sum situations (where actions benefit everyone to some degree) or negative-sum situations (where actions hurt everyone to some degree), everything from the cold war to sporting events have engrained in our thinking that everything has a winner and a loser and everything balances out.
This mentality is deeply rooted in our psyche and is even something we don’t self-identify, which makes it difficult to even notice in our thoughts and behaviors. As such, it is often unchallenged and since we don’t know we are doing it, we make no effort to recover from it. It makes it difficult to build action plans let alone be successful with those plans. Even efforts to train on experience will struggle, if it isn’t called out and addressed.
In PX, this is often seen in that every benefit that a patient gets from a healthcare experience comes at the cost of a staff member. This sentiment is captured in a conversation that I have had with Chief Nursing Officers and Chief Medical Officers repeatedly across the country.
CNO/CMO: How do we address patient experience?
Joe: Start with the traditional must-haves of hourly rounding, bedside shift reports, whiteboard validation, collaborative rounding, etc.
CNO/CMO: That puts an undue burden on the nursing staff so we can’t do it.
Joe: So, we won’t address patient experience then.
CNO/CMO: I am not saying that. But how do we address patient experience?
While not necessarily intentional, this conversation assumes and perpetuates the perception that patient experience is a zero-sum game, where any gains for the patient come at the cost of the clinical staff. As a result, it is difficult to find a path to create change. This tension permeates down to the frontline staff as well, who see these tasks simply as increasing their workload. This is, in part, the fault of the patient experience trainers as well, as we often approach training with an aggressively patient-focused approach, instead of reframing the conversation as win-win. In the next essay, I will discuss ways to break this cycle and build a more collaborative approach with staff. Here, though, I want to dive deeper into where this patient vs. staff dynamic comes from and how it colors how we communicate.
Like so many issues with patient experience, I think that the root of this comes from a focus on a problematic minority of interactions. I have spoken to dozens of emergency department staff and had the same conversation. They will tell me that the reason why their PX scores are struggling is because half of the people who come through the ED are drug-seekers. I will ask them how many patients came through their ED last night. When they tell me (say, 300), I will say, “Wow. You had 150 drug seekers last night?” They will say, no, perhaps it was only a third. “So, you had 100 drug seekers last night?” As we talk, we come to see that
- There are drug seekers who come into the ED and they are persistent, clever, and hostile and as a result they take up a lot of staff’s attention.
- After awhile it is hard to NOT see everyone coming in, especially those with ill-defined pain, as a possible drug seeker until otherwise informed.
The reality is that humans are bad at math, but good at sentiment. They are pattern-sensing animals, who for thousands of years needed to determine if the rustle in the grass was the wind or a lion. Natural selection meant that those who always assumed LION were more likely to survive. Not all patients are drug-seekers, but by assuming that, staff can have defenses up and protect themselves.
Of course, this approach to patients also means you are setting a tone—explicit or implicit—with everyone you meet and it certainly establishes a very clear first impression. Less obvious, perhaps, is that your first impression of the patient colors your patient’s first impression of you as well.
When I had my trip to the hospital that involved an overnight stay, the staff kept asking me if I was in pain. Since I didn’t know what was wrong with me and since they didn’t tell me what they thought was wrong with me, I just assumed that they were trying to determine if I was a drug-seeker, which meant that I probably underplayed my pain level because I was defensive about being pigeon-holed. I was not there for drugs, I had a real problem, even if I didn’t know what it was called.
Outside of clinical repercussions, this focus on the problematic minority has caused us to define patients in a very clear way—as problems until otherwise notified. Workplace violence is a real problem. After suffering in silence, hospitals have been publicly proclaiming that their space is violence-free and those who violate this will be dealt with severely. Signs like the one below are cropping up across the country. Please note that I mean disrespect to the state of Kentucky. These were just the first ones I found in my Google search. Kentucky is not unique in its desire to protect staff.
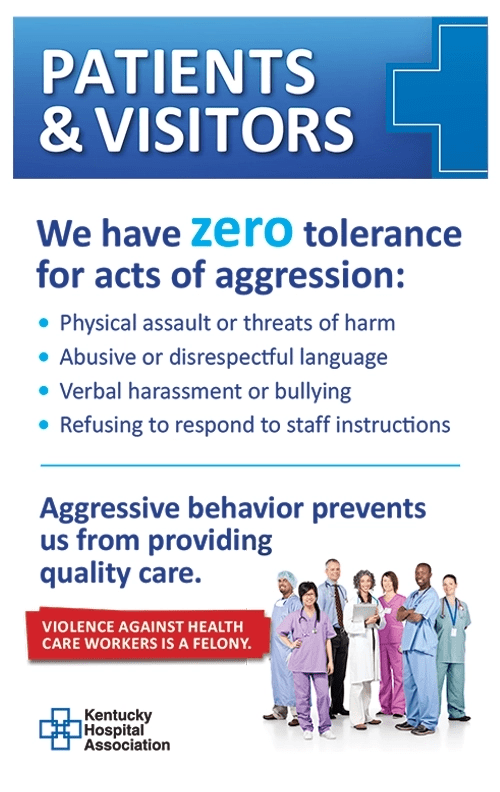
While I absolutely support all efforts to protect staff from violent patients, I have a few issues with these signs. First, they set a very clear tone and first-impression. It says that healthcare workers are under attack and their enemy is YOU. Yes, healthcare workers have been subject to violence by patients with anger issues, substance abuse problems, and mental illness. But the sign itself doesn’t draw any distinctions. It doesn’t say, “While most patients are great, there are a few bad apples.” It says you are seen as a potential problem until otherwise indicated.
Second, it is likely to be counterintuitively problematic. Is the person that this sign is really directed to going to read and internalize it? No. Far more likely is that the people who read this sign and feel its weight are the ones who don’t need the notice. In fact, these are the folks who will see phrases like “refusing to respond to staff instructions” and think that they may be kicked out because they didn’t take off their shoes or DID take off their shoes. You may think I am being silly but remember that an emergency department is an alien place with people doing weird things, often without explanation. If you have time and ability, go listen in an emergency department and see how often patients are told to do something without first being given any explanation. When I was in the ED and the staff was about to jam an IG tube into my nose and I asked them to stop and explain what was happening, was that me “refusing to respond to staff instructions”? Of course, this is not what that phrase or that sign is intended for, but it is how it can be read by patients who are scared, need help and are now told that if they say the wrong thing, they could be kicked out or worse.
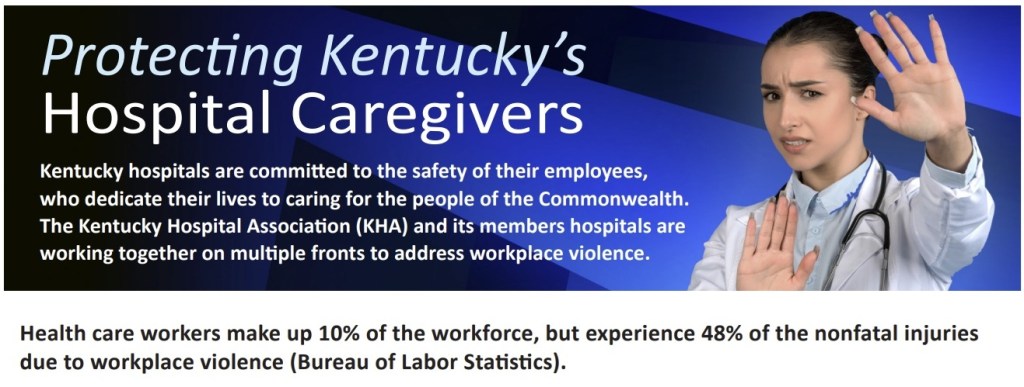
Third, and, frankly, most importantly, these signs are not inclusive. I walk into an emergency department and I see this sign. What does it tell me about this emergency department? It might tell me that this place is a shithole full of crazy people who are engaged in violent behavior. Further, it says that the hospital will take care of its own employees and you, dear patient, are on your own. The second sign opens with a statement “committed to the safety of their employees.” Would it have been so hard (or inaccurate) to say, “committed to the safety of all people in this hospital: patients, families and employees alike.” Without inclusion, you tell the patient that they are the problem. They should shut up, be docile, and that if shit meets fan, they are on their own.
Again, clearly none of this is what is intended by these signs. The problem is that these signs don’t consider how they are being viewed. I am not saying that they make patient behavior worse, but I am not convinced that they make behavior better.
At least these signs are visible and explicit. Increasingly, hospitals are adding red-flags into patient EHRs identifying “problem patients.” These are added by staff without warning or notifying the patient that they are being flagged1 and without any significant oversight. This, combined with the fact that these flags often have no expiration date, means these flags are easy to assign and difficult to remove.2 Moreover, this flag will clearly color how a staff member approaches this patient, and the patient doesn’t even know why they are being treated in such a manner.
I have already heard of cases where patients were flagged for saying, “Ow, that fucking hurts!” or one in which a patient claims that the phlebotomist told them to squeeze their hand if it would help and then flagged the patient for “squeezing too hard.” Now, it is possible that these patients are underselling their role in the red flag they were given, but without notification and due process, we really have no way of knowing what the real story is.3
I feel it necessary to state, once again, that I am in favor of strategies that will help protect staff. My concern with the messaging and use, though, is that it is a poor first impression. It is setting most interactions off on the wrong foot, and soon even the things that were designed to help will be so much white noise, to be ignored by staff.
Moreover, if staff continue to see that things designed to help patients hurt them, or things designed to help them, hurt patients, they become less able to see any PX initiative as anything other than a burden. In the next essay, I will discuss ways of breaking this cycle. For the moment, though, I encourage you to reflect upon any preconceived ideas you have that might color your ability to engage fully in your work. This includes not just patients, but coworkers. After all, your tacit opinions about those people in imaging, or in the emergency department, or in food service can certainly also color your patients’ perceptions as well. More on this to come.
1In talking with a group at a conference about this at a conference. One person told me with no indication of irony, that patients could not be told notified about this for fear of making the situation worse. Another in the group said that they already had patient complaints because another care-giver commented, “Oh, I see you have been flagged…”
2I predict that in a few short years, so many patients will carry a flag as for them to be meaningless, in the same way that if everyone is a fall-risk, no one is a fall-risk.
3For further information on this, please watch the movie, Rashômon.

Leave a comment