A big reason why the patient experience does not fully integrate with an organization’s other work is that organizations tend to focus on the wrong things when it comes to the patient experience. Whether your organization focuses exclusively on top-box scores or on Net Promoter Scores, you are likely not focusing on the patients who are most important to your overall success—the quiet ones somewhere between love and hate. In the process, not only are you failing to improve, but also you are failing to properly engage your staff in the core behaviors needed to improve.
No matter how often I show people, from senior leaders to frontline staff, their patient experience data, they are continually surprised that a vast majority of patients give them high scores. I showed the data below in a previous essay, but it is useful to show it here as well. It shows the percentiles of Promoters (9s & 10s), Neutrals (7s & 8s) and Detractors (0s thru 6s), in the HCAHPS data.
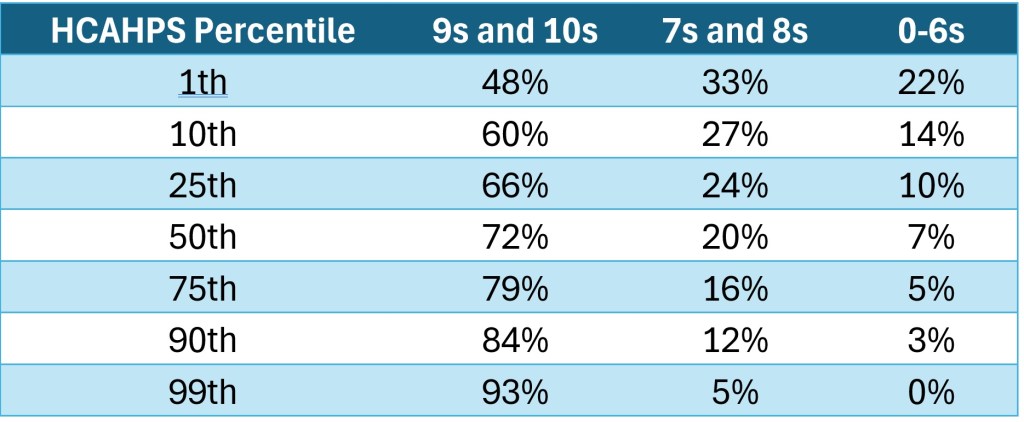
I will draw your eyes to three things in this data.
- Notice that unless you are the 0nd percentile1 hospital, the largest percentage of patients you have are those who give you 9s and 10s. So, unless you work at Abandon All Hope Ye Who Enter Here General Hospital, you are already succeeding at your PX mission more often than you are failing. Indeed, if you exceed the 1st percentile, a majority of your patients fall into the Promoter category.
- Also notice that for everyone other than that one hospital, the number of Neutral (7s & 8s) is greater than the number of Detractors (0s through 6s). So, the percentage of Detractors is the smallest for just about every hospital in the United States who submits HCAHPS data.
- By the time you get to the 10th percentile, the numbers have calmed down and the pattern in percentages stays consistent. The bad numbers go down, and the good number goes up. So, the average hospital (the 50th percentile) wins almost 75% of the time. Further, they have almost three-times more Neutral patients than they have Detractors.
- Look specifically at the Detractors. Once you hit the 25th percentile, your angry patients drop to only 1-in-10. But you will also notice that this number does not go away. It drops, as it should, but it drops slowly. Heck, a hospital at the 95th percentile still has 2% of their patients crabby. In the gap between the 25th and the 75th, the Promoters score goes up 12%, but the Detractors score only goes down 6%. Between the 50th and the 95th, Promoters score goes up 16% and the Detractors score only goes down 3%.
It is clear that most of the movement in Promoters does NOT come from reducing the number of Detractors, but from converting Neutrals into Promoters. So, why do organizations spend 95% of their energy focusing on the crabby patients? Yes, we need service recovery. Yes, we want to avoid lawsuits. Yes, we want to avoid negative reviews on Google. Yes, the squeaky wheel gets the grease. But when we care more about the crabby than the silently-satisfied, we are doing nothing to move our overall scores. When your primary PX activity is addressing complaints and responding to negative reviews, you should not be surprised if your overall 9s and 10s don’t go up.
This is because excellence is NOT the absence of problems. We don’t get to “awesome” by getting rid of all the inconveniences and irritations associated with an experience. We might minimize lawsuits, but we are not generating much positive word-of-mouth. Too often, service excellence takes its cues from a broader sales approach that focuses on a target consumer’s main concerns about committing to purchase. The idea is that if a salesman can address any main concerns, they leave the customer no choice but to purchase the product.
- “I am worried about repair costs.” Don’t be! This has the highest reliability score in the industry, plus, an extended warrantee is included in the price!
- “I am worried about the cost.” I understand, but with our financing, it will only cost you a few dollars a day. Plus, think of all the money you will save, with this efficient model that doesn’t break down!
While this may be a good way to close the deal, it doesn’t do much to build a relationship between the consumer and the seller. And yet, it seems that many organizations take the same approach to the patient experience. If we can remove all the obstacles, solve all the problems, we are assured of excellent scores. Every time you hear someone say, “If you cannot give me a 9 or 10, please tell me now…” this is someone who is treating excellence as a simple absence of problems.
Except that is not how we think. People tend to divide consumer interactions into two buckets. There are the base expectations which lead to simple satisfaction and there are the surprising flourishes which lead to remarkable experiences. In healthcare, we often think that the base expectations are sufficient to wow a patient. We cured your ailment, we fixed your broken part, we saved your life. So, the logic goes, providing a patient with quality best-practice healthcare is all that any patient could expect in healthcare. But this is just a patient’s base expectation. No one shows up at your hospital hoping that you know what you are doing. Getting that right is the mission. Getting that right prevents the state or the feds from shutting you down. Getting that right allows hospitals to survive on the reimbursement rate that they get from insurance companies, Medicare, and Medicaid. In terms of the survey, getting that right gets you a ‘7.’ The absence of problems is a base expectation.
Getting that top-box, then, is not about satisfying base expectations. It is about providing a flourish. It is about doing something unexpected and appreciated. Doing something remarkable, something special. This is where healthcare ends up tripping over its own feet. Too often, people in healthcare don’t think they should have to do anything special, and if they do, they often dumb it down to the point of simplicity and irrelevance.
Working in healthcare is hard. It is stressful. But so are other jobs. But for those in healthcare, what differentiates what they do from everyone else is that what they do is IMPORTANT. This self-defined importance is why some think that satisfying the basic expectation should be good enough. I have spoken of this before as terminal uniqueness. Given this antipathy, many in healthcare often derisively define service as “a mint on the pillow.” I find this funny, since this is said dismissively, but most in healthcare would LOVE to think of service as a mint on the pillow, since that is comparatively easy to manage, track and trend. The actual work they are asked to do to win at service is much harder.
For those who still struggle with this, let me put this in the words of any Marketing team. Quality best-practice medicine that makes the patient’s life better is what they could get from ANY hospital. What did you give them that they could only get from YOUR hospital?
Without this understanding, we miss the mark. Managing expected services and doing service recovery is NOT the same as doing something remarkable; service recovery is not service excellence. The things that make crabby people less crabby are NOT the things that make satisfied people happier.
But when this sentiment takes root in an organization, in its staff and in its leadership, it becomes difficult to see patient experience as anything other than fixing problems. It also becomes difficult to avoid this focus in our messaging, either. We know that service excellence is the sizzle not the steak. It is the differentiator. We say this all the time, but why, then, do we not act like we understand this?
Why does our messaging always sound like judgement? Yes, it is important to examine our gaps. But it is only important to do this in the service of how to close those gaps, not simply in the service of slapping wrists. I have had multiple leaders tell me that I should not bring up problems without also bringing up possible solutions. I understand the logic of this statement; don’t just complain about something without getting involved in creating a solution. But how often do our leaders do exactly the same thing? They scream down the org-chart at unsolved problems without providing solutions, or at least not show interest in the solutions people are working on. I once had a very short (but somewhat satisfying) conversation with a senior leader.
Senior Leader: “Don’t come to me with problems if you don’t have solutions.”
Joe: “I hear you. Does the same apply to you? Should you not label something as a problem without knowing a solution?”
Senior Leader: “Get out of my office.”
Now my mother will say that it was a shame that my ass is sometimes the smartest part of me and I will grant that at times my snark has not always helped me. But, at the same time, I think that calling out this messaging from senior leaders that failures will be punished, and successes will be forgotten contributes to the problem we have with both patient and employee experience.
If the only feedback a leader gets is negative feedback, that leader will either get good at deflecting or will check out. If the only time the CNO appears on a unit is to chew out the nurse leader about their failure to perform to set standards, when those elevator doors open and the CNO steps out, that leader starts preloading the excuses about the doctors, or the crappy staffing ratios, or the use of agency nurses, or, or, or, or. If they are attentive, they will make sure that they use a different excuse each time, just to keep the CNO guessing. Or, that leader will check out. They will stare blankly and nod as the CNO sounds like Charlie Brown’s teacher and when it is all over, the leader will say to her staff, “OK, now that that’s over, let’s get back to work.”
Not only does this draw attention towards the least efficient way of improving scores (fixing problems) and away from the most effective way of improving scores (connecting with our silently satisfied), but it also sends the message to staff that everyone hates us. No one is surprised when I say that people are surprised at the reality of the PX responses. But how many will look in the mirror and realize that the reason everyone thinks our patients hate us is because this is exactly how we frame PX strategies. If we focus on the gaps, the failures, the negative comments posted online, then you send the message that this is where our patients are.
Further, you are doing everything you can to demotivate staff. No one wakes up in the morning, jumps out of bed and says, “I cannot wait to get to work and hear how I FAILED the organization!” By focusing on problems and not solutions, by focusing on negative behaviors without identifying positive behaviors, you are telling your team that they are impediments to the organization’s success. They will feel beaten down and defensive. This then creates the vicious cycle where every time a patient asks for something or a senior leader visits a nursing unit, the first response in a staff member’s mind is, “Oh, here we go again!”
I do not mean to sound like a Pollyanna. There are problems that need fixing. There are gaps that need to be addressed. But when you globalize one bad comment, you are not encouraging people to try harder. Those who aren’t trying will feel the gap is too great. Even worse, those who are already trying harder will give up out of futility. There is no long-term solution if your primary message to your team is that their best is not good enough.
If you want to build a better more integrated approach to PX, it starts by focusing on the right thing.
- We are succeeding. A majority of our patients (in some cases and care settings, the number is closer to 75% or even 95%) are giving us the desired response.
- This means we do NOT suck. We do need to acknowledge that this may not be good enough to meet our goals, but we are doing well.
- Getting better than good is not the same as being bad. Our path to success is to identify the things we already do well, the things that really connect with our patients, and make building consistency around those things as our action plan.
In the end, remember that how you frame the challenge is exactly how your team will frame the challenge.
1To be clear, I wanted to go with 0th, but Microsoft word thought it should be 0nd. This is now officially more attention that the worst hospital in HCAHPS Overall Ratings terms, deserves.

Leave a comment